Article Text

Background
Rescue stenting may be needed for intracranial atherosclerosis (ICAS)-related large vessel occlusion (LVO). Balloon-expandable (BE) stent implantation often fails due to its stiffness. Balloon-expandable stent angioplasty with the dIstal support of stent-retriever (BASIS-Stent) technique is a novel technique that increases the success and safety of BE stent implantation. Our study presents our initial experience with the BASIS-Stent technique for ICAS-related LVO that requires rescue stenting and to assess its feasibility.
Method The clinical and angiographic data of acute ICAS-related LVO patients treated with the BASIS-Stent technique were retrospectively analyzed. The primary outcome was technical success, defined as successful BE stent implementation (successful deployment and satisfactory expansion). The secondary outcome was good prognosis at 90 days after the procedure, defined as a modified Rankin Scale (mRS) score of 0 to 2. The safety outcomes were procedural-related complications (ie, vessel perforation, dissection, vessel injury, distal embolism), postprocedural re-occlusion, and symptomatic intracranial hemorrhage (sICH).
Results A total of 19 patients with acute ICAS-related LVO treated at two stroke centers were included, and the median age of the patients was 62 years. Drug-eluting BE stents were successfully implanted in all patients; expanded treatment in cerebral infarction (eTICI) 3 reperfusion was achieved in all patients, no patients experienced procedural-related occlusion, and one (1/19, 5.3%) experienced re-occlusion post-procedure due to in-stent thrombus. None of the patients had sICH. Good clinical outcomes were observed in 13 patients (68.4%), and no patients died.
Conclusion BE stent implantation using the BASIS-Stent technique may be feasible and safe for treating acute ICAS-related LVO.
- Stroke
- Intervention
- Brain
- Artery
Data availability statement
Data are available upon reasonable request. No additional unpublished data are available
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Emergent stenting may be necessary in cases of acute intracranial atherosclerosis (ICAS)-related occlusion.
Balloon-expandable (BE) stents may outperform Self-expandable (SE) stents, as they are likely to achieve higher revascularization success rates and lower restenosis rates.
However, BE stents are relatively stiff, which makes it difficult for them to reach the target site.
WHAT THIS STUDY ADDS
The BASIS-Stent technique can enhance the likelihood of the BE stent reaching the target position.
It can facilitate the procedure and improve safety in patients with acute ICAS-related occlusion who require emergent stenting.
HOW THIS STUDY ADDS
This study highlights that the BASIS-Stent technique can facilitate the procedure and boost safety in patients with acute ICAS-related occlusion who need emergent stenting.
Introduction
The optimal endovascular therapy (EVT) for acute large vessel occlusion (LVO) caused by intracranial atherosclerosis (ICAS)-related LVO is unclear. ICAS-related occlusion tends to be refractory to mechanical thrombectomy (MT) and may need rescue therapy, including intra-arterial intravenous antiplatelet therapy1 2 and direct or rescue emergent angioplasty.3 4 Emergency angioplasty with balloon-expandable (BE) stent implantation may be necessary. Self-expandable (SE) and BE stents are used to treat intracranial artery stenosis. There are many differences between BE stents and SE stents, including radial strength, radial stiffness, acute or chronic recoil, and visibility on X-ray.5
BE stents typically have greater radial strength than SE stents6 do and are excellent at isolating chronic thrombi, excluding intravascular foreign material, and maintaining patency in highly calcified vessels.6 BE stents may be superior to SE stents in terms of revascularization success rates and lower restenosis rates.7 However, the BE stent is stiffer than the SE stent6 and may not easily and successfully reach the target site over the microwire. Moreover, in traditional procedural methods, repeated exchange may cause procedural-related complications such as vessel perforation8 and other unexpected complications.
The BASIS technique was proposed by Chen,9 which was called Balloon Angioplasty with the distal protection of Stent retriever. It was a novel technique for revascularization of acute ICAS-related occlusion. The essence of the the BASIS technique was compatibility between the stent-retriever’s wire and the balloon’s lumen. In our clinical practice, compatibility between the stent-retriever’s wire and the lumen of the BE stent’s balloon system was observed. Therefore, the BASIS-Stent technique was proposed in treating acute ICAS-related LVO in cases that need BE stent implantation and we assessed its feasibility and safety.
Materials and methods
Patients
Informed consent for treatment was obtained from all of the patients or their relatives. The study was approved by and conducted in accordance with the guidelines of the Ethics Committee of Zhangzhou Municipal Hospital (ID No. 2021 LWB251), and the requirement for informed consent was waived because of its retrospective nature. Patients with acute ICAS-related LVO who were treated with the BASIS-Stent technique were included. Patients were selected on the basis of the following criteria: (1) digital subtraction angiography (DSA) features indicating LVO; (2) suspected ICAS on the basis of clinical presentation and the presence of a tapered sign on omputed tomography angiography (CTA)/DSA10 or/and the ‘microcrater first pass effect’11 or/and stent-unsheathed effect12 or/and a diagnosis of culprit intracranial artery stenosis before stroke onset; and (3) underwent the BASIS-Stent technique.
Endovascular treatment (BASIS-Stent)
An endovascular procedure was performed under conscious sedation. An 8F sheath was retrogradely inserted into the femoral artery, and diagnostic angiography was performed to confirm that the acute LVO was caused by ICAS. After deployment of the guiding catheter into the ICA or VA, and intermediate/aspiration catheters were positioned at the intracranial segment of ICA or VA, the microcatheter and a microwire were navigated through the the total occlusion area into the distal patent artery, and the microcatheter was then retrieved back to the proximal segment of the occlusion site. Angiography was performed via intermediate/aspiration catheter to observe whether blood flowed through the vessel at the the occlusion site. When such flow was observed, a microcatheter ‘first-pass effect’ was verified, which indicates a high probability of ICAS-related LVO. If thrombi were identified distal to the stenotic site during the microcatheter ‘first pass effect’ test, the BASIS technique was strongly recommended,9 because this technique could prevent thrombus located at the distal occlusion site from migrating into the branch artery after expansion of the proximal stenotic site.
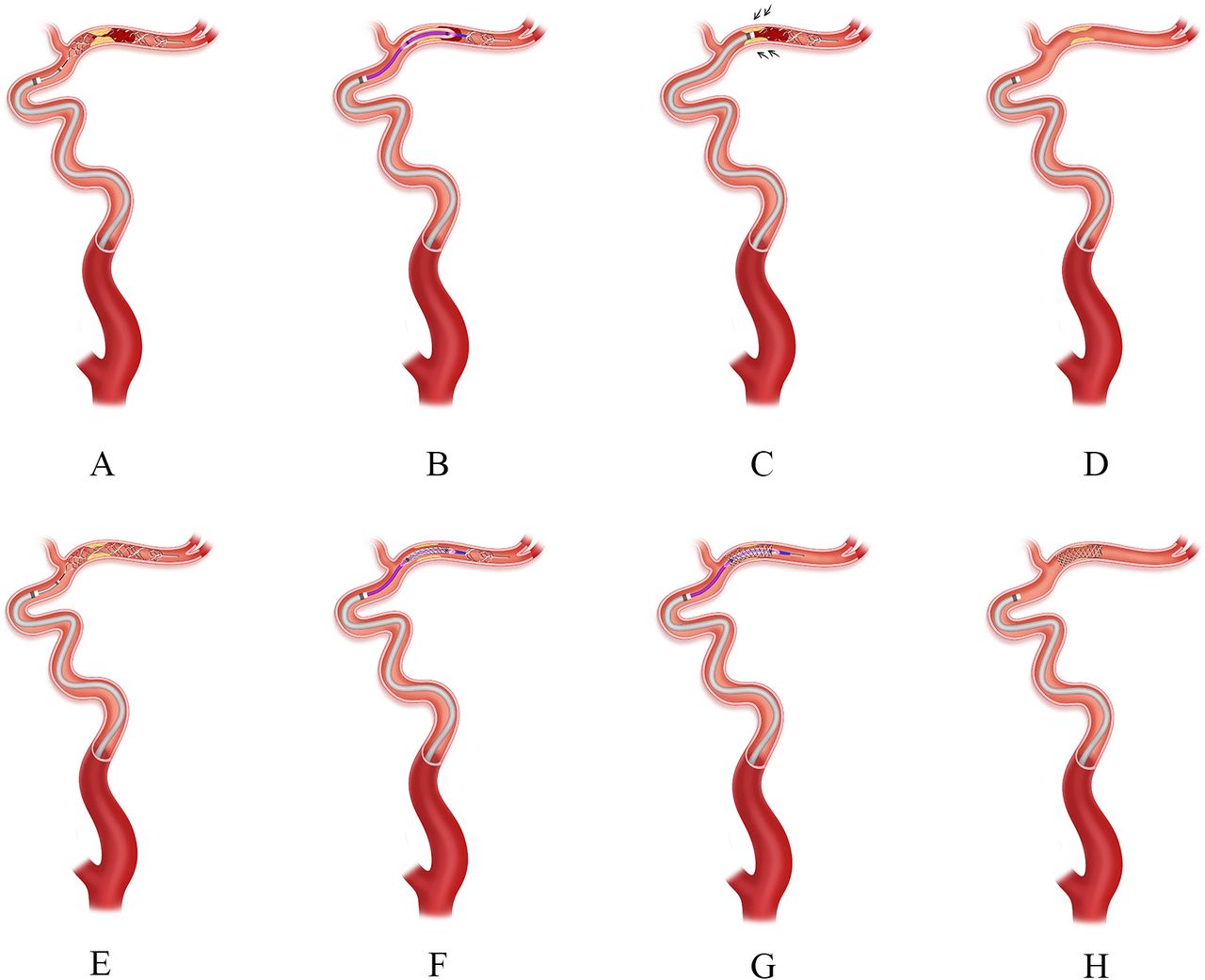
When ICAS-related LVO was confirmed, a microcatheter was navigated through the total occlusion site into the distal patent artery, the microwire was retrieved, and a stent-retriever (Achieva, China) was deployed at the occlusion site, fully covering the lesion and thrombus (figure 1A). The microcatheter was then withdrawn while the stent was in place; a suitable balloon was advanced into the stenotic site over the wire of the stent-retriever, partially retrieved stent-retriever, and inflated the balloon (figure 1B); a deflated balloon, advanced aspiration catheter close to the stenotic site. Then retrieved stent-retriever via the balloon system of the BE stent and then the stent-retriever was withdrawn under continuous manual negative pressure formed with a 50 mL locked syringe (figure 1C). Angiography was performed to determine the stenosis grade and reperfusion grade (figure 1D). If moderate to severe degree of stenosis with impaired anterograde blood flow was observed and no thrombus at the culprit artery, the stent-retriever was re-unsheathed at the stenotic site (figure 1E). Then, a suitable BE stent was advanced into the stenotic site over the wire of the stent-retriever partially retrieved stent, expanded and deployed BE stent (figure 1F). The retrieved stent-retriever via the balloon system of the BE stent (figure 1G). Angioplasty was performed to assess the blood flow and position of the stent (figure 1H).

Schematic diagram of the BASIS-Stent technique. ICAS-related occlusion of the middle cerebral artery with a thrombus formed at distal to the stenotic site. A). A microcatheter was navigated through the occlusion site into the distal patent artery, and the microcatheter first-pass effect test was used to determine ICAS-related occlusion. The microwire was retrieved while the microcatheter was located at the distal of the occlusion site and the stent-retriever, of which the diameter of the wire was 0.015 inches, was deployed at the occlusion site, which fully covered the lesion and thrombus (figure 1A). B). The microcatheter was withdrawn blindly while the stent-retriever was in place. A suitable balloon was advanced into the stenotic site over the wire of the stent-retriever and partially retrieved stent-retriever. Then, the balloon was inflated (figure 1B). C). The deflated balloon, advanced aspiration catheter close to the stenotic site, and the stent-retriever was withdrawn under continuous manual negative pressure formed with a 50 mL locked syringe (figure 1C). D). Angiography was performed to determine the stenosis grade and reperfusion grade (figure 1D). E). In the event of substantial residual stenosis with impaired anterograde blood flow, the stent-retriever was re-unsheathed at the stenotic site, F). A suitable BE stent was advanced into the stenotic site over the wire of the stent-retriever, partially retrieved stent-retriever (figure 1F). G). Expanded and deployed BE, then retrieved the stent-retriever via the balloon system of the BE stent (figure 1G); H). Angioplasty performed to assess the blood flow and position of the stent (figure 1H). ICAS indicates intracranial atherosclerosis; BE, balloon-expandable.
This procedure was performed via the following steps: (1) stent-retriever placement; (2) balloon angioplasty via the wire of the stent-retriever; (3) clot clear if there was a thrombus at the occlusion site; (4) stent-retriever replacement; (6) BE stent implantation via the wire of the stent-retriever; (7) retrieval of stent-retriever via the balloon system of the BE stent; and (8) revascularization. After step 2, angiography would be performed to check if there was a thrombus at the occlusion site, if no thrombus, step 3 and 4 would be skipped, and go directly to step 6. The novelty of this technique is summarized as follows: Balloon-expandable Stent AngioplaSty with the dIstal support of a Stent Retriever, as adopted by us, was named the BASIS-Stent technique.
Clinical and angiographic outcome assessment and measurements
The National Institutes of Health Stroke Scale (NIHSS) was used to assess patients’ neurological function, and the mRS was used to assess the clinical outcome at 90 days. Brain tissue reperfusion was assessed radiologically immediately after the operation using the Extended Thrombolysis in Cerebral Infarction (eTICI) scale, with successful reperfusion defined as an eTICI score ≥2b.13
The primary outcome was technical success, defined as successful BE stent implantation (successful deployment and satisfactory expansion). The secondary outcome was a good prognosis at 90 days after the procedure, defined by an mRS score of 0 to 2. The safety outcomes were procedural-related complications (ie, vessel perforation, dissection, distal emboli, vessel injury), postprocedural re-occlusion and symptomatic intracranial hemorrhage (sICH) diagnosed according to the Heidelberg criteria,14 re-occlusion post-procedure, which was assessed by CTA performed 24–72 hours post-procedure.
Data availability
Access to patient records for data collection and analysis was approved by our local medical ethics committee, and the need for informed consent was waived because of the retrospective nature of the study. We will share the identified data of the participants in our study on request.
Statistical analysis
The data for categorical variables are presented as absolute and relative frequencies. The data for continuous variables are presented as medians and ranges or means and standard deviation (SD). All statistical analyses were performed with IBM SPSS Statistics 22.0 (IBM, Inc., Armonk, NY).
Results
A total of 19 patients (16 men, 3 women) with acute ICAS-related LVO who were treated with the BASIS-Stent technique (illustrated case is shown in figure 2) were identified from two hospitals’ (local Municipal and local Union Hospital) prospective acute ischemic stroke database of patients who received EVT. The patients’ baseline characteristics are shown in table 1. The median age was 62 years (ranging from 54 to 70), 16 (84.2%) patients had hypertension, five (27.3%) had diabetes mellitus, two (10.5%) had ischemic stroke, two (10.5%) were smokers, and none had atrial fibrillation. The median admission NIHSS score was 12 (ranging from 4 to 17). The premorbid mRS score was 0 for all patients.

{kind=link}
{kind=link}
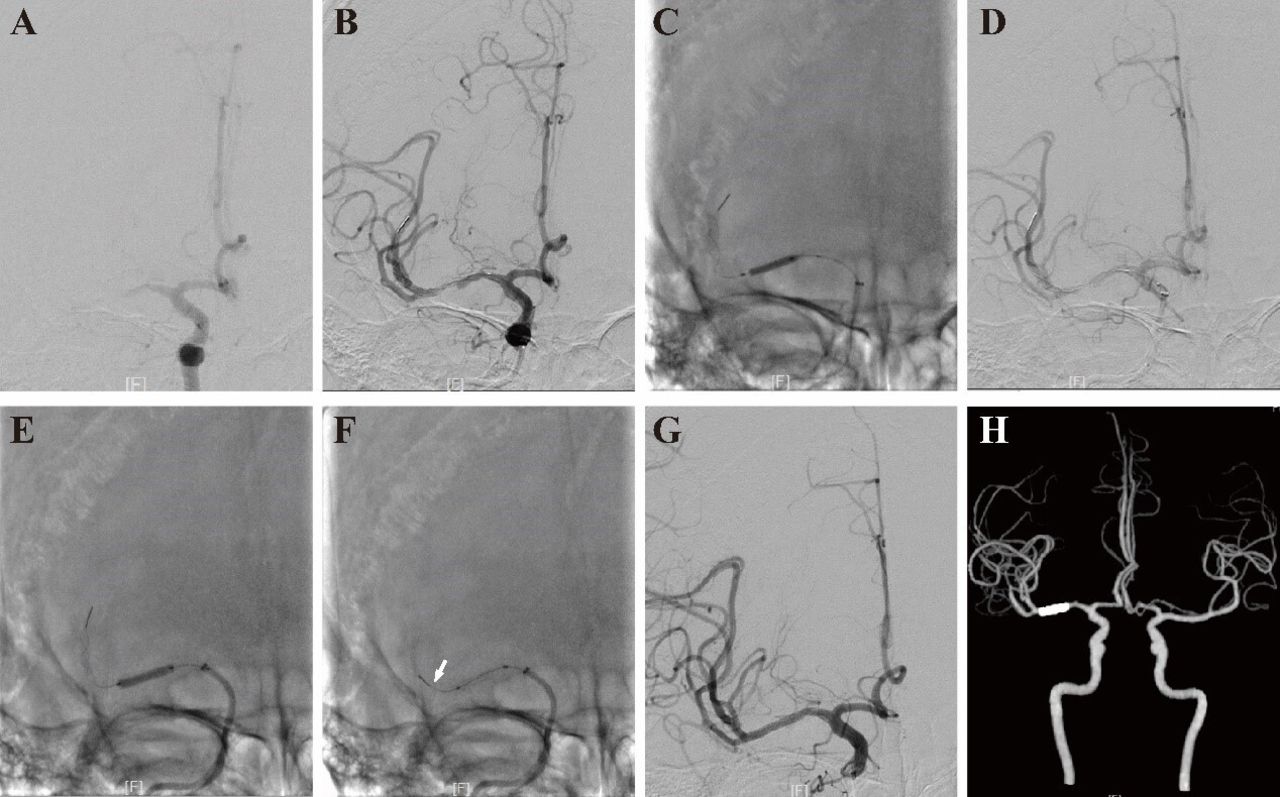
Illustrative case of the BASIS-Stent technique. A middle age male patient presented with a wake-up stroke resulting from left limb weakness for 4 hours. The admission NIHSS score was 6. (A) Right ICA angiogram showing right MCA occlusion. B). A 4–30 mm Syphonet stent-retriever was unsheathed at the occlusion site. C). A 2.0–15 mm Sacspeed neuro-balloon was advanced over the wire into the stenotic site, partially retrieved stent-retriever, and balloon angioplasty was subsequently performed. D). The degree of stenosis was relieved, but residual stenosis was severe. E). After one pass of stent-retriever, repeat angiogram showed residual stenosis was severe, then Syphonet stent-retriever was re-put at the culprit artery. A 2.5–15 mm drug-eluting balloon stent was advanced over the wire of the retrieval stent into the stenotic site, partially retrieved stent-retriever, and then BE stent was deployed via the expanded balloon. F). The Syphonet stent- retriever was retrieved via the balloon system of BE. G). Angiography revealed that the right MCA was patent without stenosis. H). Follow-up CTA revealed that the stent was in place and that the MCA was patent. NIHSS, National Institutes of Health Stroke Scale; ICA, internal carotid artery; MCA, middle cerebral artery; CTA, computed tomography angiography.
Summary of patient characteristics and clinical outcomes
The radiological assessment results, endovascular treatment outcomes, and clinical outcomes are shown in tables 1 and 2. The following vessels were detected: the internal carotid artery (ICA) intracranial segment in eight (42.1%) patients, the M1 segment of the middle cerebral artery (MCA) in six (31.6%) patients, and the intracranial segment of the vertebral artery (VA) in five (26.3%) patients. Syphonet (Achieva, China) stent-retrievers were used in all patients, and 17 (89.4%) patients underwent clot retrieval of stent-retriever, drug-eluting BE stents were used in all patients, 14 (73.6%) patients used neuro-BT stents, this included 13 (68.4%) used the Bridge (MicroPort, China) and one patient (5.3%) used the Maurora stent (Salubris, China). Five (26.3%) patients used coronary BE, this included two patients who used Proums PREMIER (Boston,USA), two used Firebirds (MicroPort, China), one used Resolute, Integrity (Medtronic,USA). Technical success and eTICI grade 3 reperfusions were achieved in all patients, and none of the patients experienced procedure-related complications. Intravenous tirofiban was administrated in all cases during the procedure bridged to oral dural antiplatelet in 15 (78.9%) patients, oral single antiplatelet in four (21.1%) patients after follow-up CT was finished after the procedure. Early re-occlusion occurred in one (5.3%) patient. None of the patients had sICH. Thirteen (68.4%) patients had a good prognosis, and no patients died.
Summary of procedural details and radiological outcomes
Discussion
The BASIS-Stent technique is a novel technique for acute ICAS-related occlusion which required BE stent implantation. This technique extends the BASIS technique reported previously.9 In ICAS-related occlusion cases, we used the BASIS technique to open the occluded artery and then implanted BE stents with the assistance of a stent-retriever in the event of severe residual stenosis with impaired blood flow. This technique is referred to as the BASIS-Stent technique.
There are several advantages of the BASIS-Stent technique. First, the successful implantation of BE stents should be increased. BE stents and SE stents are used to treat intracranial artery stenosis. Owing to its high radial strength, the BE stent was suitable for the calcified artery. Compared with those of SE stents, the rates of post-procedure stenosis and restenosis were lower with BE stents.15–17 Therefore, neuro-interventionists prefer to choose a BE stent to treat ICAS if the vessel condition allows. However, the BE stent is stiff, and 5%–10% of implantations fail (stents advanced over 0.014-inch microwires), especially in tortuous vessels.18 19 Drug-eluting coronary stents are less flexible than bare metal stents, increasing the likelihood of implantation failure.20 However, in the BASIS-Stent technique, a drug-eluting BE stent is advanced over the wire of the stent-retriever, and the supporting strength is sufficient to allow the BE stent to reach the target position due to the anchoring effect when the stent-retriever is unsheathed at distal of the artery. All the stents in our series were drug-eluting BE stents, approximately 30% of which were coronary stents, and the technical success rate was 100%, supporting the advantages of this technique. Second, the rate of procedure-related complications could be minimized. Distal vessel perforation is a serious complication that often occurs during device exchange procedures due to movement of the wire when performing this action.8 21 The BASIS-Stent technique does not involve the traditional exchange step. The stent-retriever was re-unsheathed via a microcatheter located distal to the stenotic site, the microcatheter was retrieved blindly,22 and the stent tip did not move forwards. Finally, the stent-retriever was retrieved via the balloon system of the BE stent. Thromboembolic events constitute another complication that neuro-interventionists should note and are associated with increased procedure times.21 Owing to the simplicity and easiness of BE stent implantation, the procedure time was shortened, and the incidence of thromboembolic events may decrease. Third, owing to the complex pathology of ICAS-related LVO, rescue stenting is not uncommon despite sufficient expansion via balloon.4 23–25 Therefore, the BASIS-Stent technique may increase the rate of successful reperfusion.
Some details associated with the BASIS-Stent technique should be noted. First, some specific characteristics of the device used in this technique should be noted. The success of this technique relies on good compatibility between the stent-retriever’s wire and lumen of the BE stent’s balloon system. The inner lumen of the BE stents’ balloon should allow total retrieval of the stent-retriever. Second, when the stent-retriever is retrieved via the balloon system of the BE stent, the stent cannot be fully retrieved back into the lumen of the balloon because the tip of the balloon is practically invisible. If the stent-retriever is completely retrieved back into the lumen of the balloon, vessel injury, even vessel perforation, may occur due to the movement of the tip of the balloon. Therefore, the radiopaque nature of the stent is very important,26 as radiopacity improves the successful stent retrieval rate. Third, the absence of a thrombus at the stent-retriever should be confirmed before BE stent implantation; as radiopacity improves safety of the retrival of stent retriever. Fourth, the stent-retriever could not assist multiple BE stent implantations in our series. We were not sure if the stent-retriever could be retrieved by balloon system of BE stents after implantation of multiple BE stents. Fifth, the BASIS-Stent technique can be applied in sub-acute even chronic ICAS-related occlusion.
This study has several limitations. First, the study sample size was small. However, our study is the first to present a series of cases treated at two stroke centres and to attempt to examine the efficacy of an endovascular strategy for treating acute ICAS-related LVO requiring emergency stenting. Second, the diagnosis of ICAS cannot be definitively confirmed in the emergency setting. However, our study was performed at a high-volume stroke centre and included data from more than 500 thrombectomies performed per year. The neuro-interventionists had sufficient clinical experience to distinguish ICAS from embolic cases based on clinical presentation and features on CTA and DSA, and the microcatheter first-pass effect was highly accurate for diagnosing ICAS. Third, the stent-retriever and balloon systems of BE stents are highly selected in the BASIS-Stent technique, which may influence the generalizability of this technique; however, many kinds of BE stents used in clinical practice were compatible with the Syphonet stent-retriever. Fourth, re-advancing the microwire through the stent to the distal patent artery is difficult in the event of acute re-occlusion of the stent, especially in tortuous vessels. The dilemma could be resolved if in the future the balloon system of the BE stent is designed to retrieve the stent and to allow passage of microwire.
Conclusion
This study confirms that the BASIS-Stent technique with BE stent implantation is feasible and safe for treating acute ICAS-related LVO. This technique should be considered in cases of acute ICAS-related LVO, especially in patients who need BE stent implantation.
Data availability statement
Data are available upon reasonable request. No additional unpublished data are available
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of local hospital, ID No. 2021 LWB251.Informed consent of procedure was signed by the relative of the patients, but informed consent of this study was waived by our local IRB for the retrospective study.
References
Footnotes
X @shujuan
Contributors Tingyu Yi drafted the article; Shujuan Gan, Zhiting Chen,Yanmin Wu, Dinglai Lin, Xiaohui Lin, Zhinan Pan, Lisan Zeng collected the data and created the figures; Shuyi Liu, Meihua Wu, Weifeng Huang, Yining Yang, Jinhua Ye were responsible for data arrangement and analysis; Wenhuo Chen was the guarantor, accepts full responsibility for the work, the conduct of the study, had access to the data, and controlled the decision to publish.
Funding National Health Commission capacity building and continuing education center GWJJ20221003; Beijing Health Promotion Association: Research on Appropriate Intervention Technique for High-risk Crowds of Stroke, BHPA2021IN002; Natural Science Foundation of Fujian Province (Grant No. 2022J01123162).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.