Article Text

Abstract
Background Our study aimed to investigate the relationship between the geometric distribution of plaque calcification and the occurrence of postprocedural hypotension following carotid artery stenting (CAS).
Methods We retrospectively analyzed data from CAS patients between April 2018 and February 2023. Plaque calcification was evaluated using cross-sectional images obtained from multiplanar reconstructions perpendicular to the longitudinal axis of the internal carotid artery (ICA). The cross-sectional image of the most stenotic ICA was segmented into four quadrants: interior, exterior, ventral, and dorsal. We innovatively defined the geometric classification of plaque calcification based on physiological anatomy as modified calcification location. Postprocedural hypotension was defined as persistent systolic blood pressure at <90 mmHg, requiring intravenous vasopressor infusions that lasted more than 1 hour.
Results A total of 477 patients were included in the final analysis. Among them, 41 (8.6%) patients experienced postprocedural hypotension after CAS. For the modified geometric method, plaque calcification was found significantly more frequently in the hypotension group compared with the non-hypotension group in the dorsal quadrant. Binary logistic regression analysis showed that modified calcification location on the dorsal side (OR 3.520, 95% CI 1.497 to 8.274, p=0.004) were independently associated with postprocedural hypotension after CAS.
Conclusions The presence of plaque calcification on the dorsal side, using the modified geometric method, was found to be associated with a three-fold increased risk of postprocedural hypotension after CAS. These findings may have implications for patient screening, procedure planning, and hospitalization duration expectations.
- Intervention
- CT Angiography
- Stent
- Stroke
Data availability statement
Data are available upon reasonable request. All data are available upon reasonable request. Further inquiries should be directed to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Postprocedural hypotension following carotid artery stenting (CAS) prolongs hospital stays and increases associated costs. Few studies have explored the predictive value of plaque calcification geometric distribution for postprocedural hypotension in CAS patients.
WHAT THIS STUDY ADDS
This study demonstrates that calcification on the dorsal side, identified using the modified geometric method, can predict postprocedural hypotension following CAS.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
Understanding this relationship may help identify high-risk patients, enabling clinicians to implement targeted strategies that could reduce the length of hospital stays and associated medical costs.
Introduction
Carotid artery stenting (CAS) has emerged as a safe and effective treatment option for reducing the risk of stroke in patients with carotid artery stenosis, particularly in those who are not suitable candidates for carotid endarterectomy.1–4 However, postprocedural hypotension is a common complication following CAS, with an incidence of up to 40%. This hypotension can occur as a result of baroreceptor stimulation at the carotid sinus during balloon expansion and stent implantation.5 6 Studies have indicated that postprocedural hypotension is associated with an increased risk of adverse complications, including acute renal failure, myocardial infarction, and ischemic stroke.7–9 In high-risk patients, such as those with severe stenosis or bilateral stenotic lesions, inadequate cerebral perfusion pressure can lead to the development of new cerebral infarctions.10 11 Additionally, the occurrence of postprocedural hypotension can prolong hospital stays and impose a higher financial burden.12 Therefore, the effective prediction and prevention of postprocedural hypotension after CAS are crucial for patient selection, procedure planning, and establishing realistic expectations regarding hospitalization duration.
Theoretical understanding suggests that postprocedural hypotension is commonly attributed to the carotid sinus reflex.13 The baroreceptors located in the carotid sinus are sensitive to variations in external tension.14 During stent implantation, the process of plaque compression exerts traction on the vessel wall periphery, leading to strong stimulation of the carotid sinus baroreceptors and ultimately resulting in postprocedural hypotension.15 Considering the heterogeneous response of carotid plaques to stent implantation, it becomes necessary to explore the relationship between plaque characteristics and postprocedural hypotension. This will allow for better anticipation and preparation for management.
Plaque calcification, a common pathological feature within plaques, serves as a readily accessible and straightforward evaluation marker utilizing CT. Some previous studies have explored the association between plaque calcification and postprocedural hemodynamic disorders.16–19 However, the role of plaque calcification as a predictor of postprocedural hypotension in patients undergoing CAS remains controversial. For instance, Oshin et al found that the presence of severe calcification was linked to postprocedural hypotension.18 In contrast, another recent study suggested that circumferential carotid bifurcation calcification was not a significant predictor of postprocedural hypotension.13 It seems that relying solely on calcification burden as a predictor of postprocedural hypotension in CAS patients may not be sufficient. Theoretically, based on the inherent rigidity of plaque calcification affecting the mechanical conduction of the stent and the potential specific anatomical location of carotid sinus baroreceptors, we speculate that the geometric distribution of plaque calcification may influence the progression of the carotid sinus reflex. Certain orientations of plaque calcification may have a greater propensity to stimulate the carotid sinus baroreceptors due to stent expansion. Based on these considerations, we divided the internal carotid artery (ICA) into quadrants to evaluate the impact of calcification in different quadrants on postprocedural hypotension. Understanding this relationship could help identify patients at higher risk of postprocedural CAS hypotension and potentially reduce the length of hospital stay and associated medical costs. However, currently, there are few studies investigating the predictive significance of plaque calcification geometric distribution in relation to postprocedural hypotension in CAS patients.
In this study, two geometric segmentation methodologies, the traditional geometric method and the modified geometric method, were employed to determine calcification locations. Our objective was to investigate the relationship between plaque calcification geometric distribution and postprocedural hypotension in a substantial sample size. We hypothesized that there exists an association between the geometric distribution of plaque calcification and the occurrence of postprocedural hypotension after CAS.
Methods
Ethics statement
The study protocol was approved by the ethics committee of The Second Affiliated Hospital of Zhejiang University. The study was conducted according to the principles expressed in the Declaration of Helsinki. Written informed consent for CAS was obtained from all patients or their legally authorized representatives. Because patient information was deidentified and anonymized before being released to the researchers, the informed consent requirement for this study was waived by the Institutional Review Board (Approval Number: YAN2024-1367).
Study subjects
We retrospectively reviewed data collected from patients with carotid stenosis who had undergone CAS at our single stroke center between April 2018 and February 2023. Patients with carotid stenosis involving the ICA with or without carotid bifurcation were included. The degree of stenosis was determined using the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria.20 The criteria for CAS were carotid artery stenosis ≥50% for symptomatic cases and ≥70% for asymptomatic cases.21 Patients were excluded if they had incomplete postprocedural blood pressure records, experienced restenosis after previous stenting, or lacked a computed tomography angiography (CTA) scan prior to the CAS procedure. Postprocedural hypotension was defined as persistent systolic blood pressure (SBP) at <90 mmHg, requiring intravenous vasopressor infusions lasting more than 1 hour.22
CAS procedures
All patients received a dual oral antiplatelet regimen, primarily consisting of aspirin (100 mg/day) and clopidogrel (75 mg/day), administered for at least 5 days prior to the procedure. In cases of intolerance, one of these drugs was substituted with cilostazol (200 mg/day). In emergency cases, patients were administered a loading dose of 300 mg clopidogrel and 300 mg aspirin before the procedure. CAS procedures were performed under local anesthesia via the percutaneous transfemoral route. A heparin bolus of 3000 units was administered immediately before the procedure to achieve full systemic heparinization, followed by an infusion of 1000 units per hour during the procedure. An 8F guiding catheter or a 6F sheath catheter was placed in the ipsilateral common carotid artery. Distal embolic protection devices were then deployed, and predilatation was carried out using a balloon catheter according to the vessel diameter. A stent, selected based on the anatomical and lesion characteristics, was implanted. If stent expansion was found to be insufficient, postdilatation was performed at the discretion of the neurointerventionalists. The thrombus protection devices used in CAS at our center include Emboshield NAV6 (Abbott Vascular, Santa Clara, CA, USA) and Spider FX (Medtronic, Minneapolis, MN, USA) and the carotid stents include Acculink (Abbott Vascular), Protégé (EV3, Plymouth, MA, USA), Xact (Abbott Vascular), and Wallstent (Boston Scientific, Marlborough, MA, USA). Neurological and hemodynamic status were monitored during and after the procedure. During the procedure at our center, continuous arterial blood pressure values were automatically recorded every 3 min. Additional measurements were taken promptly following balloon dilation and stent release, or if an emergency arose such as persistent hypotension. Postprocedural blood pressure values were automatically recorded using an arm cuff and sphygmomanometer every 30 min after the patient returned to the ward. Patients who developed postprocedural hypotension were treated with vasoactive agents such as dopamine. The dose was determined according to the patient’s body weight. Doses of dopamine could be increased or decreased by 2 µg per kilogram per minute based on the blood pressure readings.23
Image protocol
All CTA acquisitions and reconstructions of the head and neck were performed using a second-generation, dual-source CT system (SOMATOM Definition Flash; Siemens Healthcare, Forchheim, Germany) equipped with detectors. The CTA acquisition was performed in spiral mode with the following parameters: tube voltage 80 kV; collimation 128×0.6 mm; pitch 0.8; rotation time 0.28 s; tube current 300 mAs (CARE Dose4D); kernel B26f; ADMIRE. Intravenous access was obtained via an antecubital vein using an 18- or 20-gauge angiocatheter. CTA acquisition was performed after intravenous injection of contrast agent (40–60 mL, Omnipaque-350; GE Healthcare, Chicago, IL, USA) into a peripheral vein of the upper extremity at a weight-based flow rate of 4.5–5 mL/s, followed by a 30 mL saline chaser. Image acquisition began with a 5 s delay after a threshold of 140 HU at 120 kV was reached in the ascending aorta.
Assessment of plaque calcification distribution
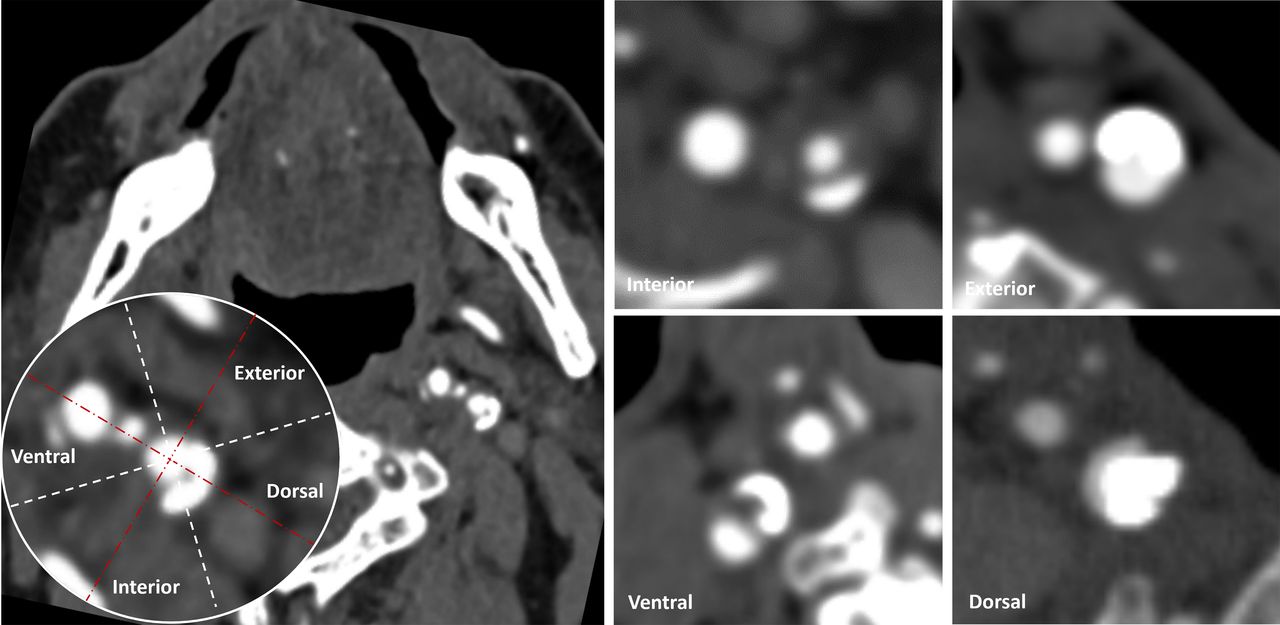
Calcifications were defined as hyperdense regions with a density of >130 HU (Hounsfield units) on CTA images.24 Plaque calcification was assessed on cross-sectional images which were perpendicular to the longitudinal axis of the ICA. The images were rotated to achieve a standard anteroposterior view. The cross-sectional image of the most stenotic ICA was segmented into four quadrants: interior, exterior, ventral, and dorsal. Conventional approaches categorize quadrants based on established geometric concepts observed in CT images, such as anterior, posterior, left, and right. However, considering the anatomical positioning of carotid sinus baroreceptors between the internal and external carotid arteries, this relationship does not fully align with conventional definitions. Therefore, it is more appropriate to define quadrants based on their orientation relative to the line connecting these arteries. Accordingly, two different geometric segmentation methodologies were employed to determine calcification locations. The traditional geometric method for identifying calcification locations relies on conventional spatial anatomy, using the vertical line (red dashed line in figure 1) as a reference. Segmentation lines (white dashed lines in figure 1) were drawn at 45° clockwise and counterclockwise, dividing the space into four quadrants (interior, exterior, ventral, and dorsal) to determine plaque calcification locations. The modified geometric method based on physiological anatomy for calcification location determination uses the line connecting the centers of the internal and external carotid arteries as the reference line (red dashed line in figure 2). Segmentation lines (white dashed lines in figure 2) were drawn at 45° clockwise and counterclockwise to divide the space into four quadrants: interior, exterior, ventral, and dorsal. A quadrant involved in plaque calcification was defined as having calcification present along more than 50% of the circumference. The number of quadrants involving calcification we also calculated, ranging from 0 to 4. Image analysis was performed by two experienced neurologists (CX and HC) who were blinded to patients’ clinical data and the inconsistent results were reviewed by another experienced neurologist (ZC) and settled by consensus discussion afterward.

A reference line (red dashed line) is used to identify calcification locations based on conventional spatial anatomy. Divided into four quadrants based on the segmentation lines (white dashed lines), plaque calcification locations can be identified in four quadrants: interior, exterior, ventral, and dorsal.

Based on physiological anatomy, calcification location determination use the line connecting the centers of the internal and external carotid arteries as the reference line (red dashed line). Likewise, segmentation lines (white dashed lines) can segment plaque calcification locations into four quadrants (interior, exterior, ventral, and dorsal) which are defined as modified calcification locations.
Statistical analysis
Clinical characteristic and imaging profiles were summarized as mean±SD or median (25th–75th percentile) for quantitative variables depending on the normality of the distribution and as frequency (percentage) for categorical variables. Fisher's exact test was used to compare the dichotomous variables between two groups, whereas an independent sample two-tailed t-test or a Mann–Whitney U test was used for the continuous variables, depending on the normality of the distribution. Associations of variables with postprocedural hypotension were determined using binary logistic regression models adjusted by characteristics with a p-value<0.1 in univariate analyses, respectively. All statistical analyses were performed using SPSS, Version 22.0 (IBM, Armonk, NY, USA). A p-value<0.05 was considered statistically significant.
Results
Overall characteristics
A total of 477 patients were finally enrolled after excluding those with incomplete postprocedural blood pressure records (n=11), restenosis after previous stenting (n=8), and lack of CTA prior to the CAS procedure (n=26). Of the included patients, the mean age was 69.3±8.4 years and the majority were male (n=411, 86.2%). The mean degree of stenosis before CAS was 70.2±14.9% with symptomatic stenosis accounting for 66.9%. Postprocedural hypotension was experienced in 41 (8.6%) patients.
Comparisons of periprocedural parameters
Compared with the non-hypotension group, the hypotension group had a shorter distance from the carotid bifurcation to the maximum stenotic lesion (7.2 vs 13.9 mm, p<0.001). The number of quadrants involving calcification was higher in the hypotension group (2 vs 1, p<0.001). There was a statistically significant difference in stent types between the hypotension group and the non-hypotension group (p=0.001). Additionally, the postprocedural duration of hospital stay was longer (4.0 vs 2.6 days, p=0.004) and medical expenses were significantly higher during hospitalization (Chinese Yuan (CNY) 3059 vs 2497, p=0.037) in the hypotension group compared with the non-hypotension group. For the conventional geometric method, calcification in the dorsal quadrant was significantly more frequently observed in the hypotension group than in the non-hypotension group (61.0% vs 19.7%, p<0.001). Moreover, using the modified geometric method, calcification was found significantly more frequently in the hypotension group compared with the non-hypotension group in the interior quadrant (43.9% vs 21.8%, p=0.001), exterior quadrant (46.3% vs 26.6%, p=0.007), and dorsal quadrant (58.5% vs 15.6%, p<0.001). No significant between-group differences in other periprocedural characteristics were identified (table 1).
Comparisons of characteristics between patients with postprocedural hypotension and those with non-hypotension
Relationship between calcification location and postprocedural hypotension
For the conventional geometric method of calcification location, binary logistic regression analysis including distance from carotid bifurcation to the maximum stenotic lesion, stent type, presence of calcification, number of quadrants involved in calcification, and calcification in the dorsal side showed that calcification in the dorsal side (OR 0.966, 95% CI 0.430 to 2.169, p=0.933) was not an independent predictor of postprocedural hypotension after CAS.
For the modified geometric method of calcification location, binary logistic regression analysis showed that distance from carotid bifurcation to the maximum stenotic lesion (OR 0.856, 95% CI 0.799 to 0.923, p<0.001), stent type (OR 1.767, 95% CI 1.079 to 2.892, p=0.024), number of quadrants involving calcification (OR 1.938, 95% CI 1.140 to 3.294, p=0.015), and calcification in the dorsal side (OR 3.520, 95% CI 1.497 to 8.274, p=0.004) were independently associated with postprocedural hypotension after CAS (table 2).
Binary logistic regression analyses for predicting postprocedural hypotension after carotid artery stenting
Discussion
The findings of our study indicate that the presence of calcification on the dorsal side, based on the modified geometric method, is an independent risk factor for postprocedural hypotension following CAS. Consistent with previous research, the distance from the carotid bifurcation to the maximum stenotic lesion and number of quadrants involved in calcification were also associated with the occurrence of postprocedural hypotension after CAS. Besides, we also found that the stent type is independently related to postprocedural hypotension. Notably, patients who experienced postprocedural hypotension had significantly longer hospital stays and higher medical expenses compared with those without this complication.
Postprocedural hypotension is a common complication observed during the periprocedural period in patients undergoing CAS, and it is believed to be caused by the stimulation of the baroreceptors located in the carotid glomus near the carotid bifurcation. Previous studies have reported varying incidences of postprocedural hypotension, ranging from 10.6% to 42.4%, which can be attributed to differences in the definition of postprocedural hypotension.6 10 13 17 25 In our cohort, 8.6% of the patients who underwent CAS procedures experienced postprocedural hypotension. Postprocedural hypotension was less prevalent in our study, possibly attributable to a larger sample size and stricter definition, which required the use of vasoactive drugs like dopamine to maintain blood pressure after the procedure.
From a pathophysiological perspective, hemodynamic instability, including postprocedural hypotension following CAS, is believed to occur due to the activation of the baroreflex in the region of the carotid sinus.26 Blood pressure regulation is tightly controlled by reciprocal changes in vagal and sympathetic neural activity, which are influenced by the baroreceptors located in the carotid sinus.27 When the carotid sinus baroreceptors are stretched and stimulated during balloon dilation or stent deployment, the stimulation of the carotid sinus leads to the inhibition of sympathetic neurons in the nucleus tractus solitarius, resulting in a reduction in sympathetic tone to peripheral blood vessels and a subsequent decrease in systemic blood pressure.28–30 Most of the hemodynamic instability occurs during the balloon dilation and stent deployment phases of the CAS procedure. Since the carotid artery stent is a self-expanding stent, a balloon is typically used for predilation and to compress the plaque before the stent is deployed. The mechanical tension exerted by the balloon on the vascular wall leads to significant stimulation of the carotid sinus. Once the stent is released, it exerts circumferential expansion forces on the vascular wall, resulting in sustained hypotension.
In the current study, we observed a negative correlation between the distance from the carotid bifurcation to the maximum stenotic lesion and postprocedural hypotension following CAS,which is consistent with findings from previous research. A study by Nanto et al also identified carotid bifurcation to maximum stenotic lesion distances of ≤10 mm as independent risk factors for developing hypotension after CAS.13 Anatomically, the carotid bulb is a dilated segment of the ICA that originates from the common carotid artery.31 When a self-expandable stent is deployed at the stenotic lesion, a maximum force of dilatation may exert greater tension on the vascular wall at the maximum stenotic lesion. That may explain why postprocedural hypotension is more frequently observed in patients with a maximum stenotic lesion near the carotid bifurcation. Specifically, for every 1 mm decrease in the distance from the carotid bifurcation to the maximum stenotic lesion, the odds of postprocedural hypotension increased by approximately 16.4%.
Furthermore, we also found that the type of stents used in CAS procedures was significantly different between the two groups in this study. We found that Xact stents were significantly more frequently used in the non-hypertension group than in the hypotension group (33.9% vs 17.1%,p=0.001). Conversely, the frequency of Acculink stents in the hypotension group was significantly higher than in the non-hypertension group (41.5% vs 17.2%, p=0.001). It is speculated that the difference in the intrinsic property of the stent cell design and the radial force of the stent might impact hemodynamics following CAS. In comparison with the Xact stents, the Accuink stents provide increased radial force.32 This increased radial force exerts a greater outward pressure on the vascular wall, leading to enhanced stimulation of the carotid sinus and subsequent activation of the sympathetic nervous system, ultimately resulting in postprocedural hypotension.10 32
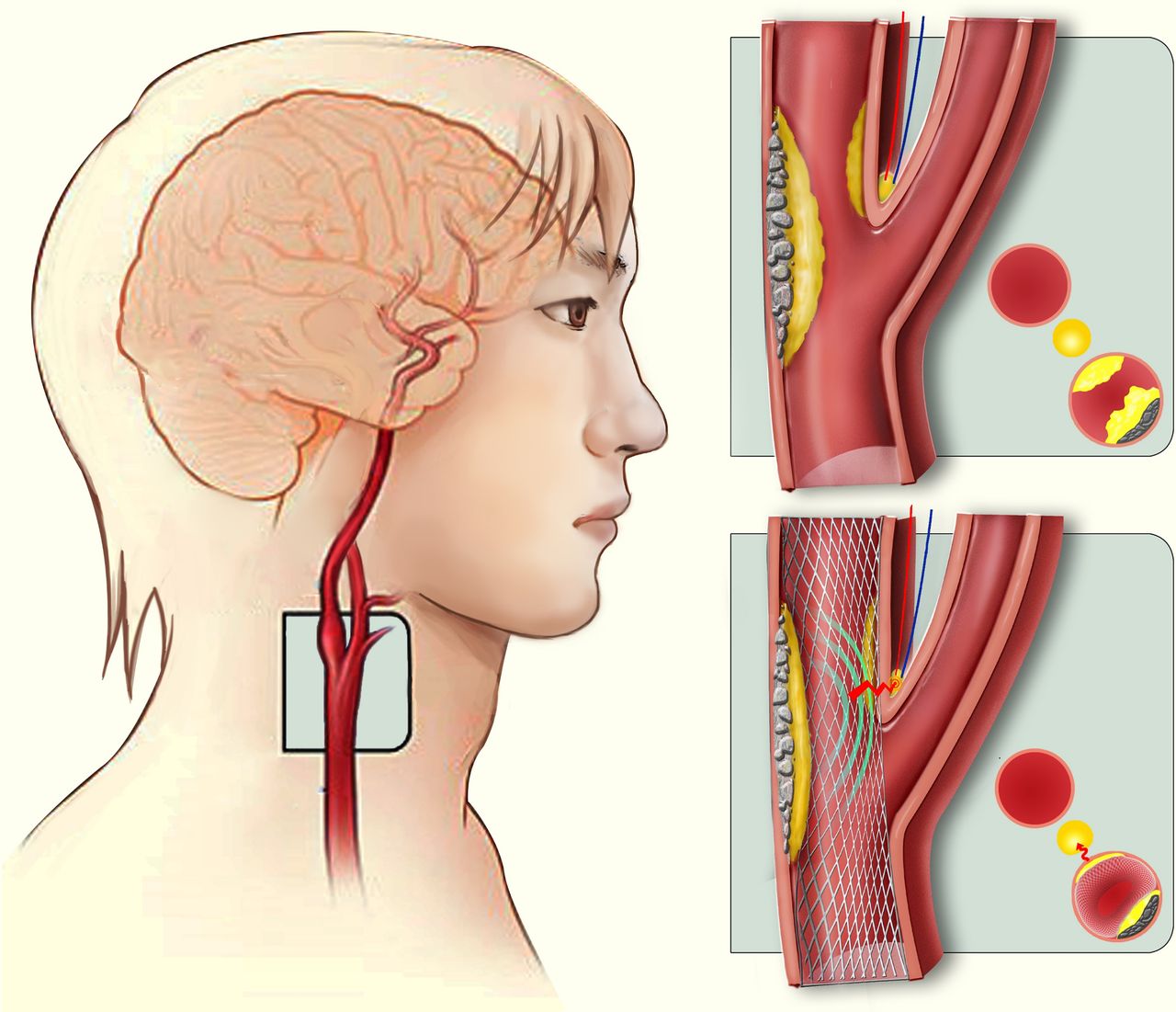
Of note, our study revealed that calcification in plaques on the dorsal side was associated with a three-fold higher risk of postprocedural hypotension after CAS. Calcification is a late-stage process in the development of atherosclerosis and is commonly observed in carotid plaques with moderate-to-severe stenosis.33 It has been proposed that calcification at the carotid bifurcation reflects local luminal hardening, which could hinder stent expansion to some extent. Chi et al found that annular plaque calcification in the carotid sinus, representing the burden of calcification, was an independent risk factor for periprocedural hemodynamic disorders.16 Another observational study also demonstrated that plaque calcification at the carotid bifurcation was associated with postprocedural hypotension.17 The main difference between our study and previous studies lies in the focus on the geometric features of calcification rather than solely considering the burden of plaque calcification. Interestingly, we found that conventional anatomical definitions of dorsal calcification are not associated with postprocedural hypotension following CAS. Anatomically, the carotid sinus nerve, originating from the glossopharyngeal nerve, runs along the anterior aspect of the ICA and innervates the carotid sinus.14 It is in the adventitial layer of the carotid bulb of the ICA.31 In theory, when a balloon is expanded or a stent is released, the expansion force is transmitted to the vessel wall. Calcification on the dorsal side may impede balloon expansion and stent release, thereby redirecting the expansion force towards the carotid sinus baroreceptors located on the ventral side of the ICA (figure 3). This altered force distribution could lead to postprocedural hypotension following CAS. As a matter of fact, the internal and external carotid arteries of patients were not strictly distributed according to conventional anatomical definitions, but rather were skewed to some degree. This may explain why only the modified definition of plaque calcification on the dorsal side is related to postprocedural hypotension following CAS.

{kind=link}
{kind=link}
{kind=link}
Schematic diagram illustrating how dorsal calcification transfers radial force from a stent to a carotid sinus baroreceptor on the ventral side during the carotid artery stenting procedure.
Our findings also revealed that individuals experiencing postprocedural hypotension had extended durations of hospitalization and incurred elevated healthcare expenditures throughout their inpatient care. A significant factor contributing to the prolonged hospital stays is the necessity for administering vasopressor medications to patients with postprocedural hypotension. The geometric arrangement of plaque calcification on CTA, a conveniently accessible and dependable imaging indicator, holds potential for identifying those individuals at an increased risk of developing postprocedural hypotension following CAS, which helps in selecting appropriate stents to mitigate post-CAS hypotension. Moreover, this assessment technique can be effortlessly implemented in clinical settings.
It is crucial to acknowledge several limitations inherent in our study, as they may influence the interpretation and generalizability of our findings. First, our study was conducted at a single center and employed a retrospective design, potentially introducing a selection bias. Second, the individual selection of stents by the neurointerventionists may have also led to a selection bias. Third, the analysis of bradycardia was not included due to incomplete data, despite its relevance as carotid sinus stimulation can result in both peripheral artery vasodilation and bradycardia. Therefore, the comprehensive investigation of the impact of plaque calcification on postprocedural hemodynamic instability may have been limited. Fourth, it is worth noting that the overwhelming majority of patients are male, which may limit the application of the findings to female patients. Finally, we did not explore the influence of different preprocedural antihypertensive regimens on postprocedural blood pressure, which warrants further investigation.
Conclusions
The current study highlights the significance of plaque calcification in the pathophysiology of CAS-induced hemodynamic instability. Enhancing our understanding of this relationship can empower clinicians to implement proactive measures aimed at reducing the occurrence of postprocedural hypotension. However, to validate our findings and enhance generalizability, larger prospective studies conducted across multiple centers are warranted.
Data availability statement
Data are available upon reasonable request. All data are available upon reasonable request. Further inquiries should be directed to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the study protocol was approved by the ethics committee of the Second Affiliated Hospital of Zhejiang University, School of Medicine (YAN2024-1367). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
ZC and HC contributed equally.
Contributors ZC: data collection for the whole trial, analysis and interpretation of data, drafting/revising the manuscript for intellectual content. HC: cleaning and analyzing the data, revising the manuscript for intellectual content. QZ: clinical data collection. SY: image data collection. PW: monitoring data collection for the whole trial, revising the manuscript critically for intellectual content. CX: study concept/design, study supervision, revising the manuscript critically for intellectual content, final approval of the version to be published. All the authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CX is responsible for the overall content as guarantor.
Funding This study was supported by the supported by Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (2023KY495, 2023KY455, 2024KY017, 2024KY752, 2025KY835).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.