Article Text

Abstract
Background and Purpose Embolization is the first-line treatment for dural arteriovenous fistulas (dAVF). The precipitating hydrophobic injectable liquid (PHIL) embolic agent is a non-adhesive copolymer with specific features and endovascular behavior. This study assessed its safety and efficacy in a prospective real-life cohort.
Methods The PHIL-dAVF study was a prospective single-arm open-label observational multicenter study conducted between October 2017 and November 2019 in 14 European centers. Patients with a single intracranial dAVF intended for PHIL embolization were included. Previously partially treated or multiple dAVFs were excluded. Additional devices and embolic agents were permitted as complementary techniques or second-line strategies. Primary endpoints were functional outcome changes from baseline and complete cure rate at 3–6 months after the last embolization. Safety was assessed by adverse events (AE) incidence.
Results A total of 67 patients (77 endovascular procedures; 70.1% men, mean age 61±14 years) were included. Most DAVFs were unruptured (71.6%), located in the transverse/sigmoid sinus (53.7%) and Cognard grade III or IV (56.7%). Sixty patients (89.6%) received one single embolization. Additional devices were used in 31.2% of procedures. Complete angiographic cure rate was 86.9% at the 3–6 month DSA follow-up after the last endovascular treatment. At least one AE was recorded in 37.3% of patients during follow-up, of which 52.9% were related to the procedure. The procedural rates of AE and serious AE were 32.5% and 15.6%, respectively. Five AEs were related to PHIL. Transient functional deterioration occurred in three patients (4.5%), all resolved by the last follow-up.
Conclusion The PHIL-dAVF study provides evidence about the efficacy and safety of PHIL in the treatment of intracranial dAVFs, with outcomes comparable to existing liquid embolic agents reported in the literature.
- Fistula
- Liquid Embolic Material
- Intervention
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Embolization is the first-line treatment for dural arteriovenous fistulas (dAVFs).
Available liquid embolic agents are effective, but may have various technical, efficacy, and safety profiles.
Precipitating hydrophobic injectable liquid (PHIL) is a recently developed non-adhesive embolic agent, offering singular physical and chemical properties compared with alternative embolic agents.
WHAT THIS STUDY ADDS
This prospective multicenter study confirmed the safety and efficacy of the PHIL embolic agent in real-life practice, achieving an angiographic cure rate of 86.9% at 3–6 months.
The study highlights PHIL’s potential in the treatment of dAVFS, including complex dAVFs (eg, Cognard grades III–IV) and in combination with complementary techniques (including pressure cooker) and devices.
The study also reported a reasonable incidence of adverse events.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings support the use of PHIL as a safe and effective embolic agent for dAVF treatment.
PHIL represents a relevant and appropriate therapeutic option in the treatment of dAVFs.
Introduction
Intracranial dural arteriovenous fistulas (dAVFs) are acquired arteriovenous shunts with a wide spectrum of clinical presentation, such as intracranial hemorrhage, headaches, focal neurological deficit, pulsatile tinnitus, cognitive disorders, intracranial hypertension, and so on. Treatment indication relies on a number of factors, including ruptured status, angiographic features and its associated risk of rupture (Cognard’s and Borden’s classifications), localization and symptoms severity.1 2 Endovascular treatment is the most considered approach through arterial, venous or both routes.3–5 In this field, embolization with liquid embolic agents is now broadly considered as a first-line approach in the majority of cases.6 7 Indeed, non-adhesive liquid embolic agents have resulted in substantial increase in the occlusion rates of dVAF.8
The precipitating hydrophobic injectable liquid (PHIL) embolic system (Microvention, Aliso Viejo, California, USA) is a non-adhesive liquid embolic agent composed of a co-polymer (polylactide-co-glycolide and polyhydroxy-ethyl-methacrylate) combined with dimethyl-sulfoxide (DMSO).9 Radiopacification is mediated through an iodine component (triodophenol) chemically bonded to the copolymer. Several concentrations are available with variable viscosity (low viscosity, 25%, 30% and 35%). Technical specificities of the PHIL embolic agent are its distinct endovascular behavior in comparison to ethylene-vinyl alcohol embolic agents, the absence of required preparation before injection, the absence of potential skin coloration and its lower degree of imaging artefacts.
Despite some recent publications, additional evidence with the use of PHIL embolic agent in the treatment of intracranial dAVF is needed.10–12 The aim of this multicenter prospective study was to investigate the safety and efficacy of the PHIL embolic agent in this indication.
Methods
Study design and population
The PHIL-dAVF study (NCT03317821) was a European prospective multicenter single arm and open label study conducted in 14 centers (France, Spain, United Kingdom, Denmark, Sweden) between October 2017 and November 2019. Inclusion criteria were as follows: (1) one dAVF that has never been previously treated; (2) the dAVF was intended for embolization with PHIL, with or without use of additional embolization devices except other non-adhesive liquid agents (Onyx or Squid); and (3) signed informed consent was obtained from the patient or their legal representative. Exclusion criteria were: (1) multiple dAVFs treated during the same endovascular procedure; (2) any condition preventing patient follow-up and participation in another study evaluating another medical device, procedure or medication during the same period. This study was an observational study following the sites’ current practice. The study received the approval of the CPP Sud-Est VI, Clermont-Ferrand ethics committee (ID: AU 1346). Patient data were collected in accordance with the requirements of the International Conference on Harmonization Guideline for Good Clinical Practice. All patients signed an informed consent form for personal data processing.
Study endpoints
The primary angiographic efficacy endpoint was the rate of complete cure at 3–6 months after the last endovascular treatment, evaluated by corelab. The primary clinical endpoint was the functional outcome at 3–6 months after the last endovascular treatment, measured with the modified Rankin Scale (mRS) and evaluated by an independent neurologist. The primary safety endpoint was the rate of adverse events (AE) at 1 month after each endovascular treatment, evaluated by the Clinical Events Committee.
Secondary endpoints included AE at 3–6 months after the last endovascular treatment, an evaluation of the quality of life (using the QOL EQ-5D score) and the symptomatic status of the dAVF.
Treatment and follow-up
Included patients were treated with an endovascular approach, under general anesthesia. Transarterial, transvenous or both endovascular routes were used, according to dAVF location and angioarchitecture, on a case-by-case basis and at operator discretion. A DMSO-compatible catheter was navigated until the embolization site (a microcatheter, a detachable-tip microcatheter or a compliant balloon). The embolization catheter was then flushed with DMSO to fill in the dead space before injection of the PHIL embolic agent. The PHIL was then progressively injected until the targeted vessels were occluded and/or the embolic agent did not penetrate adequately the targeted vessels. The formulation of the PHIL embolic agent used was left to the operator’ discretion (PHIL LV, PHIL 25%, PHIL 30% or PHIL 35%). Several arterial feeders and/or draining veins could have been treated during one endovascular procedure. In all included patients, the PHIL embolic agent was used as the first-line embolic agent. However, adjunctive techniques, agents and devices were authorized if deemed necessary to improve the likelihood of embolic agent penetration into the dAVF (pressure cooker technique with coils into an arterial feeder or with PHIL injection through a balloon), to achieve a complete cure with another embolic agent in cases of minor residual arteriovenous shunt after PHIL injection, to preserve the venous sinus patency (including the use of balloons or stents) or to control proximal arterial flow. Several endovascular procedures were performed if deemed required to eradicate the dAVF.
A first follow-up was scheduled at 1 month after each endovascular treatment, by standardized phone interview, to assess neurological status and potential AE. At 3–6 months after each endovascular treatment, patients underwent clinical assessment and angiographic follow-up with digital subtraction angiography (DSA).
Collected data
Baseline data were collected, including demographic, location and grade (according to the Cognard classification) of the dAVF, the pretreatment clinical status and the clinical presentation (ruptured or not, detailed symptoms). The following procedural data were gathered for each endovascular procedure: number of arteries and/or veins catheterized and their anatomical location, the PHIL injection duration and volume in each feeder, the use of any additional device or material (glue, coils, protection balloon, etc), radiation dose, the degree of angiographic exclusion at the end of the procedure and intraprocedural complications. Functional status, any additional treatment (new embolization, neurosurgery, radiosurgery) and the degree of occlusion of the dAVF were collected at discharge and during standard of care follow-ups. Any adverse events were collected during the overall study period.
Statistical analysis
All patients included and treated with PHIL during the study were analyzed. Categorical variables were described by their frequency distribution and ranges (bilateral 95% confidence). Continuous variables were described by their average, minimum SD, maximum, or median and quartiles. Outcomes (3–6 months cured (yes/no) or improvement of mRS at 1 month (yes/no)) were described by their distribution frequencies and intervals (bilateral associated 95% confidence).
The intention to treat (ITT) population consisted of all who signed the written informed consent and were considered to meet all inclusion/exclusion criteria (patients included in the study) following the ITT principle of whether patients received or did not receive the liquid embolic agent, PHIL. The Full Analysis Set (FAS) population consisted of all patients included in the study who received at least one embolization procedure with the use of PHIL. The per protocol set (PPS) population consisted of all subjects who received at least one embolization procedure with the use of PHIL and met all inclusion/exclusion criteria. Outcomes were evaluated in the FAS and PPS populations.
Results
Study population
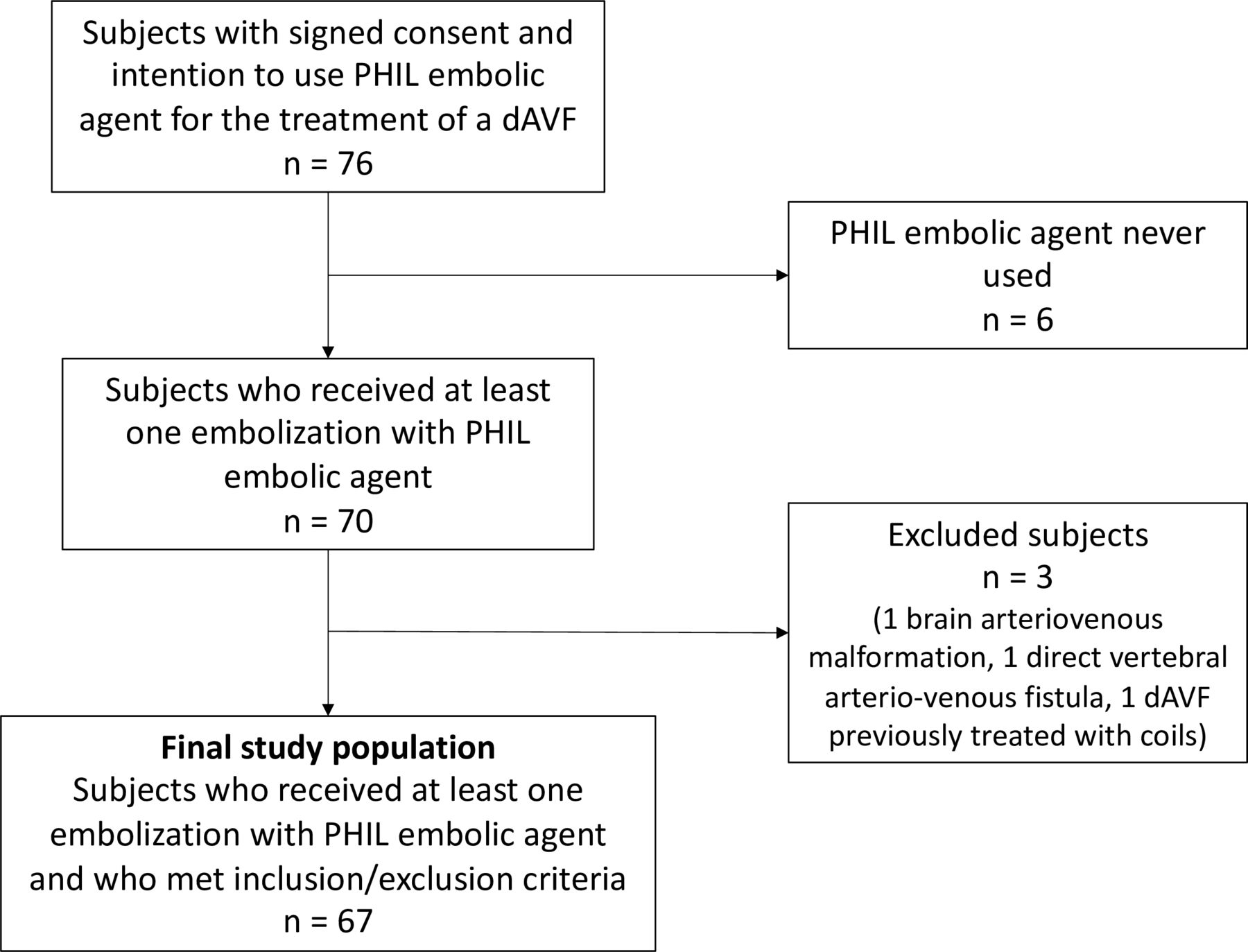
A total of 76 patients were included during the study period in 14 European centers and constituted the ITT population. Among them, the liquid embolic agent PHIL was not used in six patients, resulting in 70 subjects in the FAS population. Three additional patients were wrongly included according to inclusion/exclusion criteria (one patient with a dAVF already previously treated with coils and two patients actually not presenting with any dAVF (one brain arteriovenous malformation and one vertebral arteriovenous fistula)). The remaining 67 patients constituted the PPS population (see figure 1, study flowchart).

{kind=link}
Study flowchart. dAVF, dural arteriovenous fistulas; PHIL, precipitating hydrophobic injectable liquid.
Baseline characteristics of the PPS population are presented in table 1 and of the FAS population in the online supplemental table 1. Briefly, included patients were mostly men (n=47; 70.1%) with a mean age of 61 (SD=14). Dural AVFs were mostly unruptured (n=48; 71.6%) and only 7.5% (n=5) were asymptomatic. The most frequent location of the treated dAVF was transverse/sigmoid sinus (n=36; 53.7%). Twenty-seven (40.3%) and 11 (16.4%) subjects presented with type III and IV dAVFs according to Cognard Classification, respectively. At baseline, 44 (65.7%) had a mRS grade of 0 or 1.
Supplemental material
Baseline and procedural characteristics in the per protocol study population
Procedural and device data
Among the PPS population, all patients received at least one embolization session with PHIL. One single procedure was performed in 60 patients (89.6%) whereas 5 patients had two procedures, one patient had three procedures and one patient had four procedures. In total, 77 procedures were performed within the study. Details of endovascular treatments are presented in table 1. The endovascular approach was mostly transarterial. A total of 99 arterial pedicles were embolized (1.3 artery per embolization session) and 11 veins were treated (0.1 vein per embolization session). Most of the catheterized arteries were the middle meningeal artery (n=58) and the occipital artery (n=23). The most frequent catheterized vein was the transverse/sigmoid sinus vein (n=6). Overall, the duration of the PHIL injection lasted on average 19.6 min per arterial pedicle (range 2–80 min) and 13.6 min per embolized vein (range 2–32 min). The mean volume of PHIL injected was 1.85 mL (SD=1.52) per embolized artery and 1.74 mL (SD=1.76) per embolized vein. Additional devices were used in 31.2% (n=27/77) of procedures: coils from a venous access (n=8), pressure cooker technique from an arterial access using coils (n=4) or balloon (n=2), balloon for venous protection (n=5), balloon for arterial flow control (n=4), Squid embolic agent (n=2), glue (n=1) and venous stenting (n=1).
Angiographic and clinical follow-up
Angiographic follow-up at 3–6 months after the last endovascular treatment demonstrated a complete occlusion in 86.9% (n=53/61; six missing imaging for corelab assessment) of the study population (see table 2 and online supplemental table 2). In particular, among dAVFs of type IIa and higher, the rate of complete cure was 91.3% (n=42/46).
Outcomes in the per protocol study population
At the 1 month follow-up after the first embolization, three patients (4.5%) (all with dAVFs type>IIa) had a deteriorated neurological status (two patients with initial mRS=0 shifted to mRS=1 and one with initial mRS=1 evolved to mRS=2). Transient neurological worsening was related to seizure due to venous thrombosis induced by the endovascular treatment (n=3) and transient diplopia after embolization (n=1). All of these regressed during follow-up. During the 3–6 month follow-up after the last embolization, no patient had a deteriorated functional status in comparison to baseline. At the last follow-up, 79.1% (n=53/67) had a mRS of 0 or 1 while the 14 remaining had a final mRS between 2 and 5. No patient deceased during study follow-up. Median quality of life EQ-5D increased to 80 (IQR 70–90) at the 3–6 month follow-up.
Adverse events
At least one AE was observed for 37.3% (n=25) of patients during the first month after each embolization session, accounting for 34 AEs. Among all AEs, 12 were considered serious. Given the 77 endovascular procedures performed during the study, the respective procedural rates of AEs and SAEs were 32.5% and 15.6%. The most frequent AEs were seizures (n=2, 5.8%), cranial nerve damage (n=3; 8.8%) and urinary tract infection (n=3; 8.8%). AEs were unrelated to PHIL in 76.5% (n=26/34). Five AEs/SAEs were judged to be related to PHIL (two cranial nerve damage, one sensory deficit, one visual impairment and one superficial cutaneous occipital inflammation). A majority of AEs were considered to be certainly related to the procedure (n=18/34; 52.9%). Most AEs resolved without sequelae (n=23/34, 67.6%). Nine delayed AEs were recorded (1 month after the last endovascular procedure), including four serious AEs (one headache, one cranial nerve deficit, one renal colic and one surgery of an aorto-iliac atheromatous aneurysm). All the delayed AEs resolved without sequelae.
Eight procedural technical complications were reported. In two cases, a premature detachment of the distal tip of detachable-tip microcatheters occurred, before any embolic agent administration, without clinical consequence. In one patient, the operator faced an early occlusion of the balloon used for PHIL injection, without distal penetration of the embolic agent into the arteriovenous shunt, requiring changing the endovascular approach to a venous treatment with coils. A distal fragmentation of the embolic agent into the venous draining system was noticed in three cases, without any angiographic or clinical adverse consequence in all cases. One air embolus during a contrast injection was reported. Only the complication air embolus was symptomatic.
Discussion
In this multicenter prospective study, endovascular treatment of dAVF with PHIL liquid embolic agent achieved a rate of complete cure of 86.9% at 3–6 month follow-up after the last embolization, within one single endovascular procedure in the majority of cases (89.6%). Of note, complementary devices or additional embolic agents were used in about a third of the procedures. The functional outcomes and safety profile were encouraging, with a stable or improved mRS at the end of the study follow-up in 95.5% and five adverse events imputed to the embolic agent.
Since the therapeutic breakthrough permitted by the development of liquid embolic agents, the endovascular approach is established as the first-line strategy in intracranial dAVF treatment. Evolution of embolic agents and devices has allowed the rates of complete cure to increase.5 8 In the present study, the observed occlusion rates after dAVF embolization with PHIL liquid embolic agent were in line with recent publications.7 13–16 The result of the PHIL-dAVF study confirmed the encouraging previously published preliminary results, based on smaller case series with this embolic agent.10–12 17 Also, occlusion rates reported in the available literature regarding dAVF embolization with an alternative liquid embolic agent such as Onyx or Squid range between and 68.5% and 90.9%.5 6 13 16 18 19 These findings suggest that the endovascular singular behavior of the PHIL might lead to comparable efficacy to ethylene vinyl-alcohol copolymers.
Another point of interest in the present study was the wide variety of endovascular strategies, approaches and devices in which the PHIL was used for dAVF embolization. These included transarterial or transvenous approaches, pressure cooker techniques with balloon, coils or glue, or the use of balloon protection in venous sinus.4 9 20–22 This probably illustrates the integration of the PHIL embolic agent within the modern therapeutic arsenal of dAVF. The absence of sedimentation phenomenon, its specific radiopacity based on a bonded iodine component and the neutral color without potential tattooing effect in superficial vascular structures are singular properties of the PHIL liquid embolic agent.9 In combination with encouraging efficacy and safety, these characteristics might also influence indications and operator’s choice.
The safety profile was also consistent with recently published data in the field. Twelve SAEs were reported in this study. Five AEs/SAEs were finally considered related to the liquid embolic agent, including neurological deficits and superficial cutaneous inflammation. Despite being relatively rare, these events are identified to be potential complications in dAVF treatment and might not be specifically related to the type of liquid embolic agent itself. These procedure related events have already been reported with alternate embolic agents, with comparable rates.5 13 15 18
We acknowledge several limitations. First, this study design was single arm observational and open label. Selection bias in the study population cannot be excluded. Differences between participating centers in treatment decisions and endovascular approach including additional devices and embolic agents might have influenced the results. The number of included subjects might be perceived as limited but identifying a substantial study population was challenging given the relative rarity of dAVFs. Long-term follow-up was not available as the last visit planned in the study protocol was the 3–6 month angiographic and clinical follow-up after the last embolization session. Although low in number, there were a few missing data. Yet, several strengths of this study may be underlined. These comprised the corelab evaluation of angiographic endpoints, the prospective data collection and monitoring, and the centralized adjudication of AEs by a clinical events committee.
Conclusion
The PHIL-dAVF study investigated the efficacy and safety of the PHIL embolic agent in the endovascular treatment of intracranial dAVF. This study reported encouraging results regarding occlusion rates, functional outcomes and complication risks in a real-world prospective setting.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by CPP Sud Est VI, Clermont-Ferrand, ID: AU 1346. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Collaborators PHIL-DAVF study investigators: Blanc Raphael, Saleme Suzana, Berge Jérôme, Marnat Gauthier, Mengeon Patrice, Cognard Christophe, Moret Jacques, Aleu Bonaut Aitziber, Guimaraens Leopoldo, Parrilla Guillermo, Zamarro Parra Joaquín, Garcia-Villalba Blanca, Vivas Diaz Elio, Saldaña Jesus, Gil Alberto, Ortega Quintanilla Joaquin, Piotin Michel, Mounayer Charbel, Barreau Xavier, Januel Anne-Christine, Spelle Laurent, Casasco Alfredo, Espinosa De Rueda Mariano, Guimaraens Leopoldo, Gonzalez Garcia Alejandro, Holtmannspötter Markus, Bendorf Götz, Keston Peter Mark, Lobotesis Kyriakos, Cronqvist Mats, Borota Ljubisa, Boccardi Edoardo, Valvassori Luca.
Contributors I certify that all authors have contributed to the present study: subject inclusions, data collection and manuscript revision. In addition to previous tasks, GM and CC specifically analyzed the results and drafted the manuscript. GM is the guarantor.
Funding This study was funded by Microvention.
Competing interests GM: consulting fees (Microvention Europe, Balt SAS, Stryker Neurovascular), paid lectures (Cerenovus, Phenox, Penumbra, Bracco, Medtronic); XB: consulting fees (Microvention Europe, Balt SAS, Stryker Neurovascular); PK: consulting fees (Microvention Europe, Phenox, Stryker Neurovascular); EB and LV: advisory board (Microvention Europe); CC: consulting fees (Microvention Europe). The others authors have no conflict of interest to declare.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.